
Update
Following the recent announcement that twice weekly Lateral Flow Tests will be offered to everyone in England, it’s worth reiterating a couple of things.
Firstly, Lateral Flow Tests are for people with no symptoms. If you have any Covid-19 symptoms it is really important you get a PCR test, and that you and your household isolate while you wait for the results.
Secondly, if you get a positive result on the Lateral Flow test, you need to get a PCR test done to confirm the result. You and your household must isolate while you wait for the results. A positive PCR confirmation means you need to continue to isolate.
Finally, regular, repeated LFTs will go some way to detecting asymptomatic Covid-19 carriers and minimising the spread. However, a negative test is not a guarantee that you are Covid-19 free, so mask wearing, social distancing and avoiding contact with vulnerable people should be maintained.
One of the areas where I keep coming across a lot of misinformation relates to Covid-19 testing. I covered all the various misconceptions surrounding polymerase chain reaction (PCR) testing, including what it can and can’t detect, whether there are lots of false positives and whether the inventor of PCR really said PCR shouldn’t be used to test for Covid-19 (from the grave!) in my previous article. Please have a read if you missed it.
In this article I want to focus on Lateral Flow Tests as they are a fairly recent addition to the testing arsenal in the UK, with schools and certain workplaces having begun routine testing of everyone in the last month. It is believed that part of the UK’s roadmap out of lockdown will involve all adults testing themselves twice a week.
So, what is a Lateral Flow Test, how well does it work and how should the results be used in the weeks and months ahead? Let’s take a look…!
“What is a Lateral Flow Test?”
Covid-19 Lateral Flow Tests, which work in a similar way to a pregnancy test, are used to detect a piece of the Sars-Cov-2 virus (which is the virus that causes Covid-19), often a bit of protein from the outside of the virus. Watch here for a short video explaining how these tests work.
LFTs are used to determine if someone is currently infected with the virus. They are not as good at giving a positive result in an infected patient as PCR is. However, they are quick and cheap, and they provide a useful mass testing method in schools or workplaces.
“I’ve heard that the results of LFTs aren’t reliable, so what’s the point of using them?”
It’s always worth remembering that diagnostic tests are rarely, if ever, 100 per cent accurate. The day or time the sample is taken may not be optimal, the way the sample is taken may not be perfect, the processing of the sample might also have issues, and the test itself may not be 100 per cent perfect in what it does or does not pick up.
If you think about a pregnancy test (another form of LFT), a negative result may be caused by taking the sample too soon after conception to register a positive result or taking it at the wrong time of day when the concentration of the pregnancy hormone is too low in the urine. A similar thing applies to the Covid-19 LFTs. If you take the test too soon after infection, or when the infection is waning, you are more likely to get a negative test result.
The quality of the sample will also have a big impact. It is not an especially comfortable experience to push a testing swab up your nose and into the back of your mouth, and you have to be quite disciplined to brush the swab around for the requisite ten circles of each tonsil and each nostril! There will undoubtably be some negative results due to not picking up enough virus in the sample.
The processing of the sample may also have issues. Particular techniques are suggested to ensure that as much of the sample swab material ends up in the testing solution. But people in a hurry, or not used to dealing with small amounts of fluid in little medical supply tubes, may not take as much care to do this step correctly as they need to.
The accuracy of the tests themselves have been analysed using multiple studies now. It is worth noting that not all Covid-19 LFTs were created equal, as this review shows! The ability of different branded tests to detect a true positive case varied between 34 and 80 per cent. They all had a greater than 99 per cent chance of correctly identifying a true negative case.
For this article I will use the data from the Department of Health and Social Care published report on Innova LFTs, the brand being used in the UK at present for mass screening. They found the Innova LFTs had a specificity (ability to correctly detect a negative sample) of 99.97 per cent and a sensitivity (ability to correctly detect a positive sample) of 50.1 per cent.
This suggests that the test being used in schools is very good at correctly identifying the people who do not have Covid-19, but not so good at picking up asymptomatic Covid-19 infections.
“I’ve heard that the positive results found in schools are all likely to be false. Is that true?”
Headlines in the British press the weekend before school children went back to school after the recent lockdown claimed “School Covid tests: positive results ‘very likely’ to be false”. Obviously, this sounds pretty alarming and raises the old ‘false positive’ narrative used by some to try and downplay Covid-19 numbers, but what does it actually mean?
To fully understand what is being said requires a bit of number crunching. Please note that I am not a statistician, but I have run these calculations past a couple of mathematicians, and they seem happy! Feel free to stay with me through the calculations, or just trust me and jump past to the FAQs.
I will use the following assumptions:
· Innova specificity 99.97 per cent
· Innova sensitivity 50.1 per cent
· Current Covid-19 prevalence (number of cases – based on ONS weekly report) is 0.29 per cent. Assuming one third of cases in children are asymptomatic, and only asymptomatic children are being tested, we will use 0.1 per cent
· Number of secondary school pupils in England: 3.4 million.
Please note – These are not actual results, merely a model using the closest known values I can find to help explain the situation. The values I have used in the assumptions can be argued up or down (and have been on twitter!) and are, in reality, probably somewhere in the middle of a range of values.
In theory, if every asymptomatic secondary school child took a test, we would expect 3,400 to be positive, based on the current Covid-19 prevalence, which is very low at the moment. By using the published specificity and sensitivity of the Innova LFTs you would expect the following results:
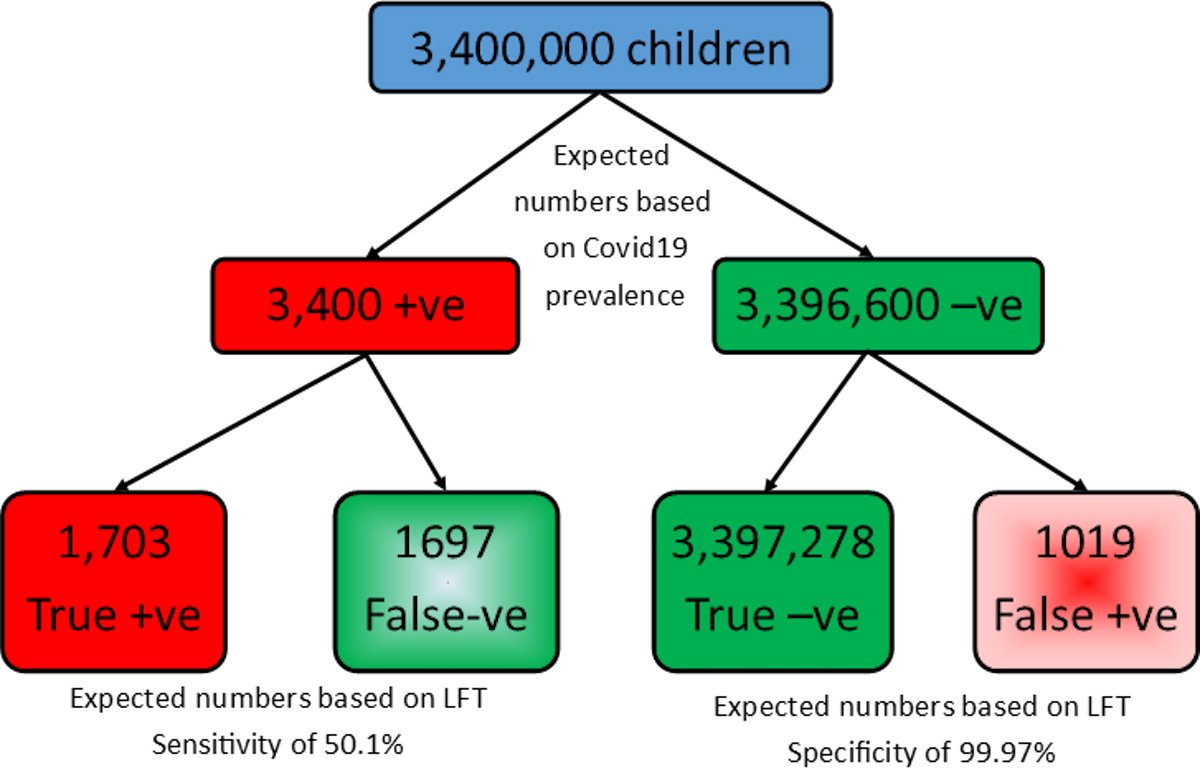
So, across England, we might expect 1,697 false negatives (a negative result in a child who does have Covid-19) and 1,019 false positives (a positive result in a child who does not have Covid-19).
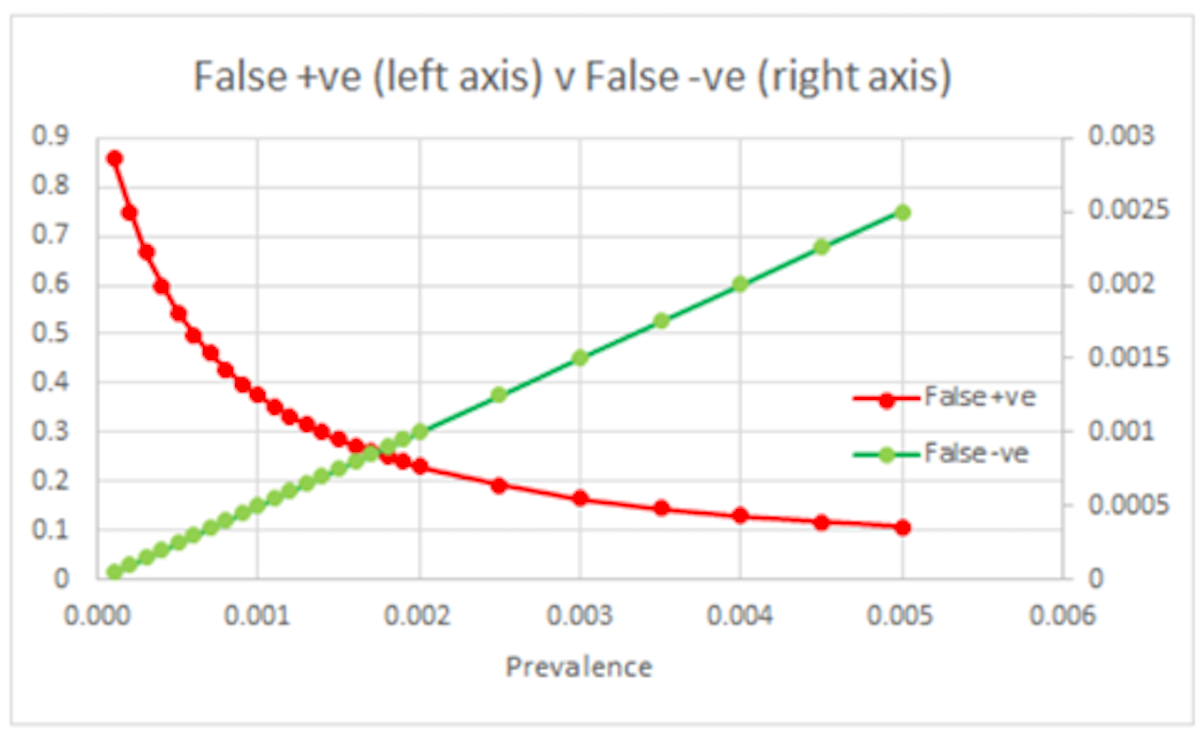
In this scenario, around 40 per cent of the positive results are actually false positives (1,019 false positives out of 2,722 positive results). When Covid-19 numbers are low, the proportion of false positives will be high. If community cases start to rise again then the percentage of false positives will decrease as more ‘true’ positives get picked up. This has been nicely illustrated by Justine Hollyer (my friendly statistician!):
Government guidelines for LFTs performed at school were that a positive result would trigger isolation for the family and no follow-up testing was required. For the children and their families who needed to isolate unnecessarily, following a false positive, this process was detrimental.
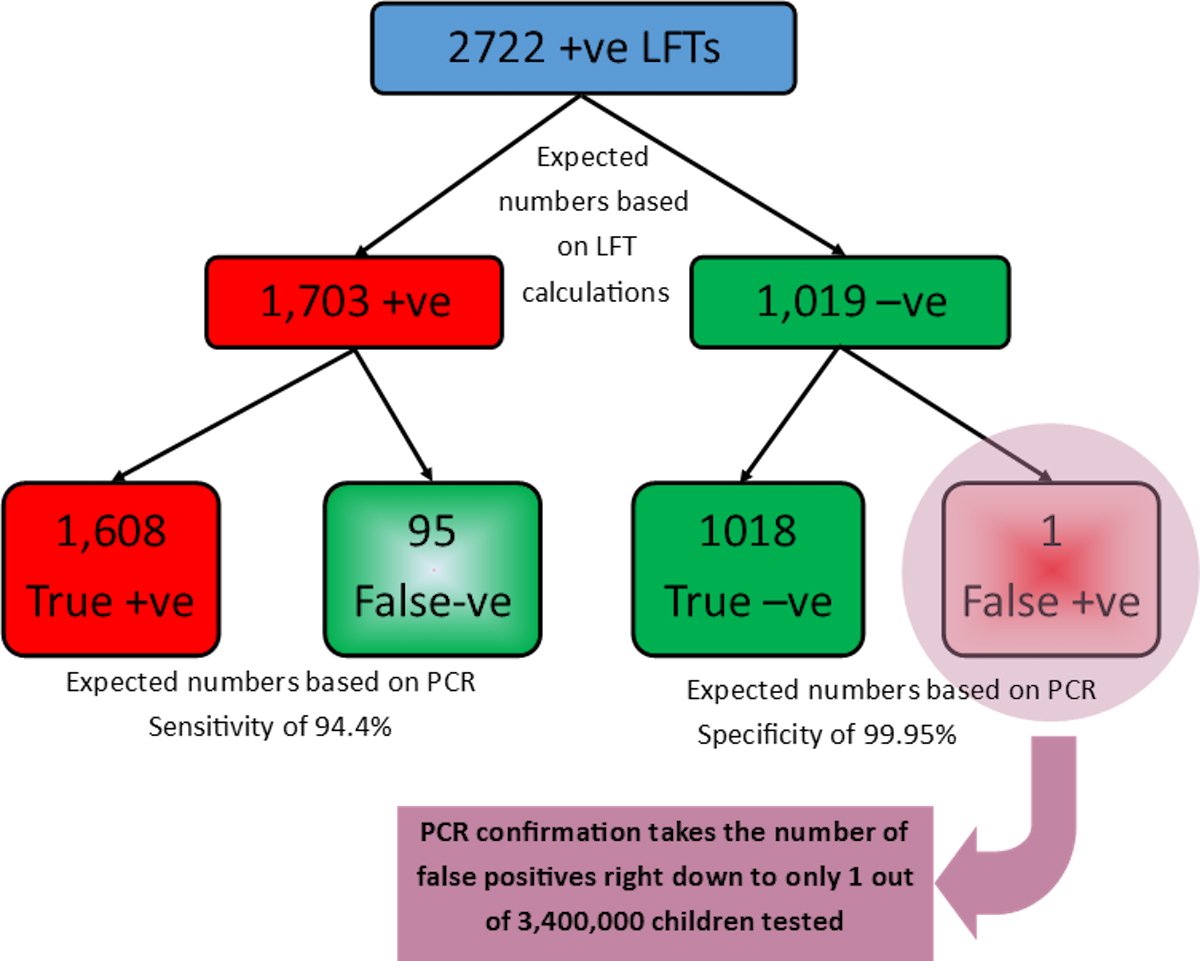
Fortunately, the policy is different now that testing is taking place at home. Any positive LFT should be followed up by a PCR test. PCR tests are incredibly good at determining whether or not the Covid-19 virus is present, with a specificity of 99.95 per cent and a sensitivity of 94.4 per cent. By taking the 2,722 positive results from the example above (1,703 true positives and 1,019 false positives) and running PCR tests on those children, we can remove 1,018 of the false positives! This means that out of 3.4 million children tested, only one child would be isolating unnecessarily, using these modelled numbers. And 1,608 children with Covid-19 will have been picked up and advised to self-isolate, to reduce the spread of the disease.
“Does that mean if I get a negative test, I don’t have Covid-19?”
Having dealt with the issue of false positives, we do need to look at false negatives (a negative result in people who do in fact have Covid-19). Using the calculations above, we can see that we would expect 50 per cent of the true positive children to give a negative test. The PCR backup of the positive cases will also ‘lose’ a number of true positives.
This is not ideal as people may feel a misplaced sense of safety following a negative LFT test. However, regular testing will make it much more likely that the false negative cases will come up as positive on a subsequent test.
At present levels of Covid-19, a negative lateral flow Covid-19 test means you have a greater than 99 per cent chance of being Covid-19 free. But if Covid-19 cases start to rise again that percentage will begin to fall. So, it’s important not to get complacent!
“Can we use Lateral Flow Tests to allow people to start going to clubs and sports venues?”
How we use these tests is really important. We know that although the vast majority of tests results will be accurate, depending on how prevalent Covid-19 is in the community, the results may miss a significant proportion of asymptomatic Covid-19 carriers. Despite these carriers showing no symptoms, we know that they can spread Covid-19 unwittingly.
So, given what we know about the accuracy of these tests in asymptomatic people, should we be using these tests to screen people? I would argue “yes” AND “no”!
In essential settings where people are going to be mixing regardless, such as in schools, care homes, hospitals etc, having this screening is really beneficial. It will pick up a proportion of infected individuals that would otherwise go undetected, and allow them and their households to isolate, thus limiting the spread of the disease. Those cases that are missed will likely be picked up several days later.
However, the idea of using these tests to allow entry into non-essential venues, particularly ones where other means of infection control are going to be missing, is a different matter. Using a test which will miss 50 per cent of true positives, to allow people to mix in close proximity in places where singing, shouting, and touching are likely, will inevitably lead to greater spread of Covid-19.

Conclusions
Used in settings such as schools, hospitals, and care homes, Lateral Flow Test screening, following up positive results with a PCR test, is a really good idea. The LFT programme’s strengths will lie in the regular and repeated nature of the testing.
On the other hand, one-off testing to allow people to mix, uninhibited, is not such a good idea and will likely lead to the spreading of more cases..
It’s important not to get bogged down in ideas of false positives and false negatives that are currently doing the rounds on social media and in the press. Well over 99 per cent of LFT results are going to give the correct result on whether or not someone has Covid-19. There will be a proportion of false positives, but PCR backup testing should all but rule them out, and there will be a proportion of false negatives, but repeated testing should catch them a few days later.
Finally, a negative result means you are more than 99 per cent likely to be Covid-19 free. So although the odds of having Covid-19 are less than one per cent, the odds of winning the lottery are far smaller and people still make that bet!
Thank you to Justine Hollyer and Alex Selby (@alexselby1770) for checking through my maths to make sure I wasn’t getting it wrong!



